


From UK-SEA Vax Hub

Explore a multitude of benefits as a member of the UK-SEA Vax Hub:
- Gain access to the hub’s expertise, knowledge, and cutting-edge technologies across three major vaccine platforms: mRNA, protein (e.g., virus-like particle), and viral vector.
- Tap into funding opportunities offered by the hub, such as business interaction vouchers and proof-of-concept funds.
- Elevate your skills through upskilling training programmes offered by the hub.
- Access materials (e.g., antigen bank) and tools developed by the hub.
- Collaborate on joint funding applications with fellow hub members.
- Engage in vaccine co-development opportunities with fellow hub members.
- Participate in cohort-based training designed for PhD students.
- Shape the landscape of vaccine development and manufacturing policies in South East Asia through your influence.

Chula Vaccine Research Center (ChulaVRC) was invited to attend the Thailand Security Dialogue 2024: “Sustainable Peace under Geopolitical Shifts”. The conference was organized by the Strategic Studies Center (SSC), the Commandant of the National Defence Studies Institute (NDSI).
Prof. Kiat Ruxrungtham, the director of ChulaVRC, shared the experience of “Vaccine Security and Equity” in the Panel Discussion session “Food and Health Security: ASEAN’s Strengths or Weaknesses for ASEAN?” This topic provided valuable information and support the ongoing efforts to enhance Food and Health Security in the ASEAN region.

From: Health Policy Watch / By Petro Terblanche, Jerome Kim, Rajinder Suri & Padmashree Gehl Sampath, et al.

Sixteen leading scientists and manufacturers involved in vaccine development and production worldwide issue an urgent call for a pandemic accord that can be a ‘win-win for all.’ The full list of authors is available below.
Health misinformation was not invented during COVID-19 but was certainly brought to a higher, more malevolent and destructive pitch during the pandemic. That hostile crusade has since been (mis)directed at two landmark agreements, the Pandemic Prevention, Preparedness and Response Agreement (Pandemic Agreement), and amendments to the International Health Regulations (IHR), that are currently being negotiated by WHO’s 194 member states for approval at the World Health Assembly.
The overarching goal of ensuring that the world will deal more equitably with the next pandemic appears to be elusive as we near the deadline of May 2024 for the close of the negotiations.
Several social media and news outlets have claimed that the WHO is negotiating two instruments that will afford the agency far-reaching powers in case of a future pandemic.
Member-state led talks

While the WHO is the global custodian of human health, the WHO is not negotiating these agreements – the 194 member states are. Aside from being untrue, the false claims undermine the goals of the Pandemic Agreement and its ability to ensure that it remains centered around the key pillars of access, equity, and global health security.
Moreover, these false claims gainsay the grim facts of the COVID-19 pandemic and the lethal consequences that the lack of equitable access to life-saving medical countermeasures imposed on the greater part of the world’s population.
The Pandemic Agreement and the IHR amendments do not grant WHO far-reaching powers and do not compel member states to surrender national sovereign rights.
Rather, they seek to ensure that, by working together, the global community can ensure the health of all. The Pandemic Agreement is an important and empowering step in that direction.
Powerful instrument for for all people
The Pandemic Agreement is a powerful instrument for mankind and, while recognising that the WHO is the internationally-recognised lead agency, it is important to remember that WHO member states initiated these processes, remain the main players in the negotiations, and are themselves, not WHO, responsible for the outcome. The World Health Assembly (WHA), not WHO, decides on the content and adoption of the agreement.
It should be borne in mind that the Pandemic Agreement is NOT written for low- and middle-income countries, but for all countries to secure health security for all peoples – rich and poor. This is critical as pandemics do not stop at country borders, nor put all within a country’s population at similar risk.
Fostering a value system that emphasises equity, as demonstrated through commitments to equal access to vaccines and therapeutics for all people, no matter who they are or where they live is central to such an outcome.
For this to happen, the agreement we need is one that will ensure access by providing a clear pathway to enable access and equity.
The world already has several instruments and treaties, such as the flexibilities under the World Trade Organization’s Trade-related Aspects of Intellectual Property (TRIPS), and the COVID-19 Technology Access Pool, now repositioned as H-TAP (Health Technology Access Programme), which have not yet been used to their full potential.
Implementation roadmap

The agreement’s success will be measured by how it can provide a better roadmap and enable more effective use of complementary agreements and instruments. We must not just discuss notions of technology access, transfer, production and equitable access but move beyond the words on paper to implementation.
There must be clarity on leadership and the need for one entity to lead and govern the implementation of the entire agreement – where health is the focus. WHO, as the directing and coordinating authority in international health work, should be empowered, and supported to effectively execute its mandate with WHO still being accountable to the WHA.
But WHO alone cannot protect the world; there are many other essential players – regional health agencies, governments, public and private agencies, funders, civil society organisations, communities, research, development entities, as well as academic and public health institutions.
Building trust for consensus amongst all these players is complex: it requires a clear view on the barriers to trust.
Moving the needle toward consensus amongst the 194 World Health Assembly states with a few days left to go will require a strong effort to eliminate the fundamental misunderstandings about the Agreement and bring forth its acceptance.
Why support a pandemic agreement?

Why should we join a movement to ensure that a pandemic agreement is agreed to by all governments and is adopted as soon as possible?
The answer is both simple and profound: in the face of the COVID-19 pandemic, people were often afterthoughts, and some countries used the worst pandemic in a century to further their own geopolitical and domestic political agendas rather than to unite to advance life-saving solutions together, effectively, efficiently, equitably, and justly both globally and within their own country.
During the pandemic, it was governments (many elected by the people) that chose – or did not choose –to impose lockdowns to quell waves of COVID-19; it was governments that chose – or did not choose – to impose travel restrictions.
When high-income countries pre-ordered far more vaccine doses than they could ever use, and indeed, millions upon millions of doses were disposed of, rather than being shared with health workers, elderly people, and immune-suppressed patients in lower-income countries when demand was high, it was governments that justified these excesses.
Act-Accelerator and COVAX partners, including the WHO, which works for its 194 member states, did their best to streamline access to vaccines, diagnostics, and therapeutics.
But WHO is only as strong as governments of the member states wish it to be – WHO cannot force governments to do anything.
A win-win for all
At present, there are several issues in the agreement still to be resolved. Higher income countries are worried about their autonomy and pharmaceutical corporations based in those, about profits, while lower-income countries in all regions, including those across Africa, are requiring mechanisms that will prevent gross inequities from recurring.
The pandemic agreement is not designed to be detrimental to the autonomy of nations or the profits of private firms but a win-win for all by preventing gross inequalities in access to vaccines, therapeutics, and diagnostics.
Some of the mechanisms being discussed involve nesting within WHO several time-bound processes that would alert governments when the first signs of a dangerous outbreak are being detected; that would require governments to share information about nascent outbreaks anywhere on the globe; whereby pandemics that threaten all people everywhere result in the equitable sharing of life-saving medical interventions – with industry, researchers, and governments agreeing in advance to a level of essential benefits-sharing that will save lives while fostering scientific innovation.

Central role of technology transfer
Paradoxically, ensuring the spread of technical know-how and manufacturing capacity to lower-income countries, which is central to these outcomes, is a strong area of disagreement amongst WHO’s Member States about the Pandemic Agreement, although the WHO has been leading an effort over the past two years to do just this.
South Africa is at the centre of this shift, and there is real hope that it will change the game for mRNA vaccine production in Africa and the use of other vaccine manufacturing technologies.
A global pandemic agreement that addresses the issue of technical know-how for manufacturing will ensure that the next time around, the global community is prepared ahead of time to accelerate this shift. Ultimately, when governments agree on principles like sharing and equity, it is ordinary people who benefit. At the same time, in the face of conflict and chaos, it is ordinary people who suffer.
A better path to global equity
To be clear, the Pandemic Agreement will not be enacted in isolation. Other established instruments, especially those that govern intellectual property and trade, will support and continue to co-exist working together to enhance access in a synergistic manner.
The agreement is a means to better address equity globally and must be owned by all governments.
We urge all of those who are curious about the Pandemic Agreement and its agreement process to learn more and join millions of others around the world to urge all governments to get the job done, to find a way to bequeath to future generations the sort of pandemic agreement which, will ensure a swifter, fairer response for a better healthier world for all.
Prof Petro Terblanche is managing director of Afrigen Biologics, South Africa, which hosts the WHO’s global mRNA technology vaccine hub.
Dr Jerome Kim is Director General of the International Vaccine Institute, South Korea.
Rajinder Suri is CEO of Developing Countries Vaccine Manufacturers Network, India.
Prof Padmashree Gehl Sampath is CEO of the Africa Pharmaceutical Technology Foundation, Rwanda.
Prof Kiat Ruxrungtham is founder and co-director of the Vaccine Research Center at Chulalongkorn University, Thailand.
Frederik Kristensen is managing director of the Regionalized Vaccine Manufacturing Collaborative and Coalition for Epidemic Preparedness Innovation.
Ramon Rao is CEO of Hilleman Laboratories, Singapore, which translates early discovery of vaccines and biologics for infectious diseases into affordable products with global health impact.
Prof Sarah Gilbert is Saïd Professorship of Vaccinology at Oxford University UK, and co-developed the Oxford-AstraZeneca COVID-19 vaccine.
Prof Glenda Gray is president of the South African Medical Research Council South Africa.
Boitumelo Semete is CEO of the South Africa Health Products Regulatory Agency, South Africa.
Prof Noni MacDonald is professor of paediatrics (infectious diseases) at Dalhousie University in Canada.
Charles Gore is executive director of the Medicines Patent Pool Switzerland.
Dr Amadou Sall is CEO of the Institute Pasteur Dakar in Senegal and Director of the WHO Collaborating Center for Arboviruses and Viral Hemorrhagic Fever.
Prof Cristina Possas is an infectious diseases expert at the Institute of Technology on Immunobiologicals (Bio-Manguinhos) at Fundação Oswaldo Cruz (Fiocruz) in Brazil.
Dr Simon Agwale is CEO of Innovation Biotech (Nigeria and USA).
Image Credits: Chris Black/WHO, UNICEF, International Rescue Committee, PMO Barbados, Kerry Cullinan.
From: Vaccine Insights
Tuck Seng Wong, Kiat Ruxrungtham
Vaccine security and self-reliance must be a priority for all nations if they are to escape the worst health and economic impacts of future pandemics. For low- and middle-income countries, this is best achieved with a wider regional approach. Existing geopolitical and economic alliances and a strong baseline of biopharmaceutical manufacturing mean that South East Asia is well-positioned to become a global leader in vaccine production. The newly launched UK-South East Asia Vaccine Manufacturing Research Hub will support this ambition by addressing key priorities including technology transfer, IP, standardization, and supply chain.
Vaccine Insights 2024; 3(2), 35–42
DOI: 10.18609/vac.2024.008

The mRNA Technology Transfer Programme organized on 18 March 2024 in Singapore the 4th Sc

From: Department of Chemical and Biological Engineering, University of Sheffield

Professor Tuck Seng Wong
Sheffield to lead £7.6 million UK-South East Asia Vaccine Manufacturing Research Hub. The Hub is a consortium of four UK universities (Sheffield, Cambridge, York and Kent) and eleven partners based in South East Asia, covering five countries (Thailand, Malaysia, the Philippines, Vietnam and Indonesia). Prof. Tuck Seng Wong at Sheffield U is the director and Prof. Kiat Ruxrungtham at Chula VRC, and School of Global Health, Faculty of Medicine, Chulalongkorn University is the co-director of this UK-SEA manufacturing research hub. “


Congratulations to Drew Weissman and Katalin Kariko
for the Nobel Prize in Physiology or Medicine 2023.
You have accomplished such a great contribution to the world.
From: The Independent Panel for Pandemic Preparedness and Response
Statement of the Right Honourable Helen Clark
Former Co-Chair
The Independent Panel for Pandemic Preparedness and Response
Opening Segment of the UNGA High-Level Meeting
Pandemic Prevention, Preparedness and Response
20 September 2023, UNHQ.
Excellencies,
Let me congratulate the General Assembly on coming together in this High-Level Meeting on Pandemic Prevention, Preparedness and Response.
Your leadership on these issues is important. You meet knowing that the COVID-19 pandemic has resulted in an estimated 24 million excess deaths, and set back progress on the Sustainable Development Goals. Many countries are still struggling to recover.
A virus we didn’t know four years ago has settled in worldwide at great cost to people and to governments.
The political declaration before you today has to be a catalyst for the change which stops this from ever happening again.
The question is, how urgently can it be built on to bring the transformation which the international system for pandemic preparedness and response requires? Viruses with pandemic potential won’t wait for years for diplomacy to produce results before they strike.
So, where do we need change?
First, on equity. Research and development, and equitable access to diagnostics, vaccines, and treatments, are issues of paramount importance to Member States. Many of us believe that these goods are so crucial to the management of health emergencies that they must be treated as part of the global commons.
There has to be a pre-negotiated and financed end-to-end ecosystem for medical countermeasures. Every region must have the technology, knowledge, and local capacity needed to stop outbreaks when and where they occur. Other essential supplies to safeguard human life must also be accessible. Bottom line: no country should be at the mercy of global markets to protect its citizens.
Second, on finance. The demand for grants from the new Pandemic Fund is vastly outstripping what is available. A global public investment model is needed to gathering the funds to support low- and middle-income countries. That should also apply to surge financing in the event that a pandemic threat emerges and rapid action is needed. Spending billions will save trillions and will protect human life and future progress on the SDGs.
Third, the Geneva processes must be ambitious. Revised International Health Regulations can help speed up detection, reporting, and alert of pathogens of international concern. WHO must be empowered to sound the alarm rapidly, with evidence, and without bureaucracy. There is no time to lose. COVID-19 spread around the entire globe within four months. That cannot be allowed to happen again.
A new pandemic accord can commit countries to strengthen national health systems, surveillance, solidarity, and equity. This is the world’s next opportunity. Please do not miss it.
Fourth, governance. The declaration before you seeks to “Strengthen regional and international cooperation, multilateralism, global solidarity, co-ordination and governance at the highest political levels and across all relevant sectors.” The question is, how will you do this?
Can a leader-level body such as that recommended by the former Independent Panel and others be established? If not now, when?
As a former Prime Minister and a former Minister of Health, I believe that a council of Heads of State and Government is needed to help break the cycle of panic and neglect and sustain political momentum for preparedness and response.
Next year’s Summit of the Future may address the management of complex crises and could present another opportunity for action for ensuring leadership at the highest level.
Fifth: accountability. Independent monitoring of country preparedness is needed to guarantee mutual assurance. Compliance and accountability with international agreements is in every nation’s interest, and is critical to protecting the most vulnerable and marginalised.
Preparedness requires working with communities and addressing misinformation and disinformation – starting now. You cannot build trust in the midst of a crisis.
I leave you with this final thought. Imagine if one of us here, now, were infected with a new, dangerous virus. More of us would become infected this week. We would fly back home to our families and communities, potentially sparking another crisis. Would our countries be ready to manage that outbreak? Would the world?
I am confident that human ingenuity and solidarity can make COVID-19 the last pandemic of such devastation.
But that is a political choice. You have the power to make it.
Thank you.
_________
For more information, contact Christine McNab: +1 416 986 2068; ChristineMcNab@gmail.com

From BioNet-Asia
ChulaCov19 BNA159 is a COVID–19 mRNA vaccine developed by Chulalongkorn University and produced by BioNet

- ChulaCov19 mRNA vaccine was found safe and immunogenic for primary immunization in clinical trials in Thailand.
- The Australian trial will evaluate the safety and immunogenicity of a booster dose of ChulaCov19 BNA159 mRNA vaccine in healthy volunteers.
- The collaborators of the trial are Chulalongkorn University, BioNet and Technovalia.
Melbourne, 15th November 2022 – Technovalia, Chulalongkorn University and BioNet today announced that Human Research Ethics Committee (HREC) in Australia approved the phase 2 trial of ChulaCov19 BNA159 mRNA vaccine as a booster dose in adults.
Ethics approval is granted to commence a phase 2 trial after sharing satisfactory results of clinical safety and immunogenicity data of prior phase 1 and 2 studies of ChulaCov19 mRNA vaccine.
Mr. Laurent Dapremont, Chief Executive Officer of Technovalia said: “We are pleased to have received ethics approval for testing the ChulaCov19 mRNA BNA159 vaccine. We have been leading the development of genetically designed innovative vaccines in Australia, starting with clinical trials evaluating a recombinant pertussis vaccine, two DNA COVID vaccines and now a mRNA COVID vaccine.”
The clinical trial will assess the safety and immunogenicity of one single booster dose of ChulaCov19 BNA159 mRNA vaccine in healthy volunteers having previously received vaccination with an approved COVID-19 vaccine. The trial includes several sites in Australia and will commence in November.
Assoc. Prof. Chanchai Sittipunt, MD, Dean of Faculty of Medicine, Chulalongkorn University added: “Our university aims at developing approaches to move society forward. Developed in Thailand, Chulacov19 mRNA vaccine has already shown good safety data and very promising immunogenicity data in Thai phase 1 and phase 2 trials. We are glad to continue its development as a booster vaccine and to sponsor this clinical study in Australia. We believe mRNA vaccines will play an important role to combat current and future pandemics and infectious disease threats.”
ChulaCov19 mRNA vaccine was developed by Professor Kiat Ruxrungtham and his team of Chulalongkorn University Vaccine Research Center (ChulaVRC), Thailand, in collaboration with Professor Drew Weissman of the University of Pennsylvania, USA. the first ChulaCov19 vaccine lot was manufactured in the U.S. and was evaluated in a phase 1 safety trial in Thailand. It was then evaluated in a comparative phase 2 safety and immunogenicity trial in Thai adults and elderly participants who received two primary doses of vaccine. The ChulaCov19 vaccine was compared to an mRNA vaccine licensed in Thailand. The new multi-centre trial in Australia, will evaluate the boosting immunity induced by one dose of ChulaCov19 BNA159 vaccine, produced in Thailand, in adults aged 18 – 64 years.
Dr. Pham Hong Thai, Chief Executive Officer of BioNet, added: “We are very pleased to collaborate with Chulalongkorn University to produce mRNA vaccines against SARS–CoV–2 and to continue our development partnership with Technovalia. We have been collaborating on several vaccines of which three are in clinical trial stage in Australia. This is a key milestone for all our colleagues who worked relentlessly towards the success of this mRNA vaccine project.”
BioNet has established an end-to-end manufacturing platform to produce mRNA vaccines from cell bank to encapsulation in record time. ChulaCov19 BNA159 mRNA vaccine is the fruit of a collaboration between Chulalongkorn University and BioNet. The mRNA technology platform enables the rapid development of new vaccines in 100 days from research to use in human trial. A second-generation mRNA vaccine against Omicron variant and the ancestral strain of SARS-CoV-2 virus is also in development.
About Chulalongkorn University
Chulalongkorn University aims to become a model institute of education, setting the standard as a university of innovations for society and focusing on three social development core principles: preparing future leaders, developing impactful research and innovation, and advocating social sustainability. The university has 20 faculties, 23 colleges and research institutes, more than 3,000 full-time faculty members and over 37,000 students. Recently, Chulalongkorn University was ranked Asia’s No.1 for Global Impact by Times Higher Education (THE) Impact Ranking 2021, which is the global performance scale that assesses universities using the United Nations’ 17 Sustainable Development Goals (SDGs). Chulalongkorn University earned the scores of SDG 3 for Good Health and Well-being and SDG 9 for Industry, Innovation and Infrastructure.
About BioNet
BioNet is a biotech organization sharing expertise and innovation to secure rapid access to vaccines. Located in France and Thailand, BioNet creates genetically designed vaccines and produces Pertagen, the world’s only recombinant pertussis-only vaccine containing genetically inactivated pertussis toxin. BioNet has also established technology platforms to produce DNA and mRNA vaccines with 10 projects in preclinical and clinical studies. BioNet is advancing global research in collaboration with eminent advisors and organizations (The Pasteur Institute, The Bill and Melinda Gates Foundation, PATH, CEPI and IVI). BioNet has developed bio-clusters fostering vaccine self-reliance around the world and for 20 years, BioNet has driven a unique manufacturers alliance deploying 10 billion doses of polio vaccines worldwide.
About Technovalia
Melbourne-based Technovalia is a privately-owned Australian biotech company dedicated to the research and development of innovative vaccines. In partnership with several academic organisations and international companies, Technovalia is investing in the development of new technology platforms that have the potential to significantly improve protection against several infectious diseasesby producing safer, more stable, and more cost-effective vaccines. Technovalia is developing BioNet’s recombinant acellular pertussis-only vaccine Pertagen® in Australia and needle-free COVID-19 DNA-based vaccine Covigen.
For further information, please contact:
Ms Michelle Tat
Marketing Communications
E-mail: info@technovalia.com


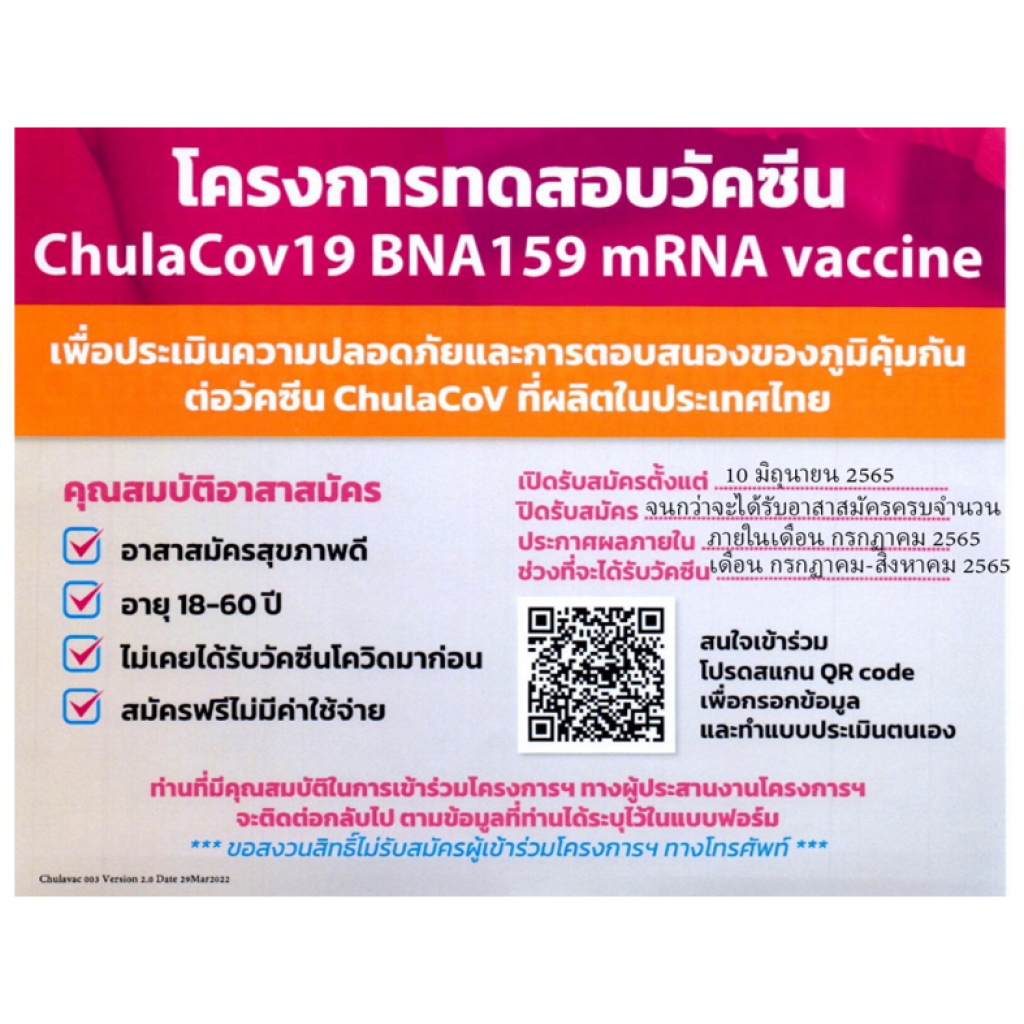
เปิดรับสมัครอาสาสมัครสุขภาพดีสำหรับโครงการ ChulaCov19 BNA159 mRNA vaccine
คุณสมบัติ
- อายุ 18 – 60 ปี
- ไม่มีโรคประจำตัว
- ไม่เคยติดเชื้อ covid19
- ไม่เคยได้รับวัคซีน covid19
เปิดรับลงทะเบียนตั้งแต่วันที่ 10 มิถุนายน 2565
สำหรับผู้ที่สนใจแสกน QR code หรือคลิ๊กลิงค์ที่ปรากฏ พร้อมกรอกข้อมูลให้ครบถ้วน
>> https://bit.ly/3I0HH8w <<


A COVID-19 vaccine made by BioNet-Asia in Ayutthaya, Thailand, should be cheaper than the two messenger RNA vaccines used in richer countries.ADAM DEAN
From: Science/ By Jon Cohen
The two COVID-19 vaccines based on messenger RNA (mRNA) have been the breakout stars of the pandemic. Both trigger impressive immune responses with minimal side effects, and both did exceptionally well in efficacy trials. But the vaccines, produced by the Pfizer-BioNTech partnership and Moderna, have also split the world. Because of their high prices and their need to be stored at extremely low temperatures, few people in lower and middle-income countries have had access to them.
That might soon change. More than a dozen new mRNA vaccines from 10 countries are now advancing in clinical studies, including one from China that’s already in a phase 3 trial. Some are easier to store, and many would be cheaper. Showing they work won’t be easy: The number of people who don’t already have some immunity to COVID-19 because of vaccination or infection is dwindling. But if one or more of the candidates gets the green light, the mRNA revolution could reach many more people.
The Pfizer-BioNTech and Moderna shots rely on mRNA to direct cells to produce spike, a protein on SARS-CoV-2’s surface. Although 23 COVID-19 vaccines are in use around the world, based on technologies including inactivated SARS-CoV-2 and cold viruses engineered to carry the spike gene, the two mRNA vaccines account for about 30% of the 13.2 billion doses produced so far, according to health care data company Airfinity. But the companies have been reluctant to share their intellectual property (IP) and know-how, which would allow manufacturers in poorer countries to produce the shots.
Instead, BioNTech and Moderna each recently announced plans to build their own plants in African countries. In a separate effort, the World Health Organization has created a training hub for mRNA vaccines that will teach scientists from low- and middle-income countries how to build and run their own plants. But it may take years before these efforts bear fruit.
The candidates already under development could reach the marketplace much faster. IP protections are still a challenge, says Melanie Saville, who heads vaccine R&D at the Coalition for Epidemic Preparedness Innovations: “Who can do what and where is going to be a critical question.” But the new mRNA developers have managed to dodge some of the showstoppers.
Furthest along is a vaccine made by Walvax Biotechnology in Kunming, China, together with Suzhou Abogen Biosciences and the Chinese Academy of Military Science. Details are hard to come by and Walvax did not respond to detailed questions from Science, but a paper about a phase 1 trial, published in The Lancet Microbe in January, offers some information. Instead of using mRNA that encodes the entire spike protein, the Walvax team only included the sequence of a key portion known as the receptor binding domain. In July 2021, the company launched a placebo-controlled phase 3 trial in 28,000 people in Mexico, Indonesia, Nepal, and China.
A key advantage is that Walvax’s product can be kept in a standard refrigerator, says Víctor Bohórquez López, a clinician who leads trials at five sites in Mexico for Red OSMO, a network based in Oaxaca. A company official told Reuters in January that Walvax can produce 400 million doses a year.
In Thailand, a team lead by Kiat Ruxrungtham at Chulalongkorn University has developed an mRNA vaccine, produced by the French-Thai company BioNet-Asia, that has completed phase 1/2 studies. The team followed a key step in the playbook used by the Pfizer-BioNTech collaboration and Moderna: replacing uridine—one of the four basic building blocks of RNA—with methylpseudouridine, a substitution that reduces the toxicity of mRNA and increases the amount of spike protein cells produce. The substitution is “the most important thing that people have done with mRNA vaccines,” says Philip Krause, a former top vaccine official at the U.S. Food and Drug Administration (FDA). BioNet-Asia can use the replacement for free because the company that licensed the technology from the University of Pennsylvania, where it was invented, has not sought protection in Southeast Asia.
A new wave of mRNA COVID-19 vaccines
A bevy of messenger RNA (mRNA) vaccines against COVID-19 are currently in clinical trials around the world. Because placebo-controlled efficacy trials are increasingly seen as unethical, some trials compare a new vaccine with a proven one (comparator). Others give the vaccine to people who are already fully vaccinated and measure the immune response (booster).
| MAIN MANUFACTURER | Country | mRNA type | Clinical phase |
|---|---|---|---|
| Walvax Biotechnology | China | Conventional | 3 (booster) |
| Gennova Bio* | India | Self-amplifying | 2/3 (comparator) |
| Vinbiocare Biotechnology** | Vietnam | Self-amplifying | 1/2/3 (comparator) |
| Daiichi Sankyo | Japan | Conventional | 1/2/3 (booster) |
| BioNet-Asia | Thailand | Conventional | 2 |
| Providence Therapeutics | Canada | Conventional | 2 |
| Arcturus Therapeutics** | United States | Self-amplifying | 2 |
| Elixirgen Therapeutics | United States | Self-amplifying | 1/2 |
| EyeGene | South Korea | Conventional | 1/2 |
| Stemirna Therapeutics | China | Conventional | 1/2 |
| AIM Vaccine Group | China | Unknown | 1/2 |
| HDT Bio* | United States | Self-amplifying | 1 |
| GlaxoSmithKline (GSK) | United States | Self-amplifying | 1 |
| VLP Therapeutics | Japan | Self-amplifying | 1 |
| Imperial College London | England | Self-amplifying | 1 |
| Gritstone Bio | England | Self-amplifying | 1 (booster) |
| University of Melbourne | Australia | Conventional | 1 (booster) |
| CureVac/GSK | Germany | Conventional | 1 |
*/** denote shared technologyDATA: WORLD HEALTH ORGANIZATION; COVID-19 VACCINE TRACKER
The vaccine differs from the marketed ones in other ways, however. Kiat’s team did not introduce two mutations in spike that stabilize the protein, which would have required an expensive IP license. They avoided another licensing issue by having the code direct cells to secrete the spike protein, rather than leaving it bound to the membrane. Some comparative studies have found this leads to a weaker immune response, but Kiat’s mouse studies saw no difference, and human data show the vaccine triggers robust levels of antibodies that can neutralize the virus, he says.
BioNet-Asia can make up to 100 million doses a year, Kiat says, at a lower price than the Pfizer-BioNTech collaboration and Moderna. Japan’s Daiichi Sankyo and Canada’s Providence Therapeutics have mRNA vaccines at similar stages of development.
About half of the new candidates are “self-amplifying”: They include harmless genes from an alphavirus that code for an enzyme used in RNA replication, enabling the spike mRNA to make additional copies of itself. Each dose can get by with less mRNA, which could make it easier to vaccinate more people. A downside is that self-amplifying mRNA vaccines can’t use the methylpseudouridine substitution—they need the natural uridine to replicate.
A phase 1 study of a self-amplifying vaccine developed at Imperial College London triggered such mediocre immune responses that the researchers went back to the drawing board. But a similar candidate from GlaxoSmithKline solidly protected hamsters against SARS-CoV-2 infection, a January paper in Molecular Therapy showed. That vaccine is now being tested in a 10-person phase 1 trial.
Showing that the new vaccines work in humans presents formidable challenges. “I’m in trouble because I can’t find the population right now for the phase 3 trial,” Kiat says. Not only is it becoming more difficult to find people who have no immunity at all against SARS-CoV-2, but enrolling participants in a placebo-controlled study is increasingly ethically fraught, because proven COVID-19 vaccines are now widely available. Producers of self-amplifying vaccines in India and Vietnam instead plan to compare the vaccines with others already in use.
Kiat hopes to judge his candidate based on a proxy measure: how well it boosts antibody levels in people who are fully vaccinated. Past studies of the marketed mRNA vaccines have shown that specific levels of neutralizing antibodies are correlated with protection from disease, and BioNet-Asia and other manufacturers hope regulators will accept similar data to authorize use of their vaccines. The European Medicines Agency and regulators from several countries have indicated they will accept such “immunobridging” data in some circumstances, Krause says. FDA has yet to issue guidelines. “I know from talking to people at FDA that they are reluctant” to rely on antibody data, says Stanley Plotkin, a veteran vaccine researcher who consults with Moderna and many other companies.
One problem is that antibodies are only part of the immune response triggered by mRNA vaccines. T cells—which are more difficult to measure—play a role in preventing severe disease by eliminating infected cells. They also offer better protection against new virus variants than antibodies and help ensure the durability of immunity. Still, Plotkin and others say, antibody levels are good enough surrogates to issue emergency use authorizations. For full approval, they say, vaccines will have to prove effective in real-world studies.
“We know that there are a lot of hurdles ahead,” Kiat says. But even if their COVID-19 vaccine fails, his team is building capacity for the future, he says. “We can now manufacture new mRNA vaccines very quickly, so that’s a way to solve the next pandemic—and we can make the price lower than the Big Pharmas.”

Dr.Chanchai Sittipunt, Dr.Nakorn Premsri, Dr.Suthipong Watcharasin and Dr.Kiat Ruxrungtham greetings to three Prince Mahidol Award 2021 laureates

Amid a global shortage of vaccines and a new wave of COVID-19 infections, some countries in Southeast Asia are rushing to develop their own coronavirus shots.
COVID19 Vaccine Tracker – Chulalongkorn University: ChulaCov19

The research team behind the development of a local mRNA Covid-19 vaccine on Monday asked the government to help finance the project

The Phase 1 trial of Thailand’s homegrown mRNA COVID-19 vaccine ChulaCOV-19, suggests the candidate vaccine can help the body elicit

The mRNA vaccine, currently being developed by the Vaccine Research Centre of the Faculty of Medicine of Chulalongkorn University, can stimulate the immune system to produce killer T-cells

The Faculty of Medicine at Bangkok’s Chulalongkorn University has put out a call for healthy volunteers to take part in trials of its Covid-19 mRNA vaccine.
